
India’s Next Medical Tourism Frontier Isn’t Cost — It’s Proven Infection Safety
May 24, 2026
How IPC excellence and AMR transparency can transform Indian hospitals into the world’s most trusted healthcare destinations
Infection Prevention | AMR Strategy | Medical Tourism | Healthcare Leadership
Global AMR Burden: Where Does India Stand?
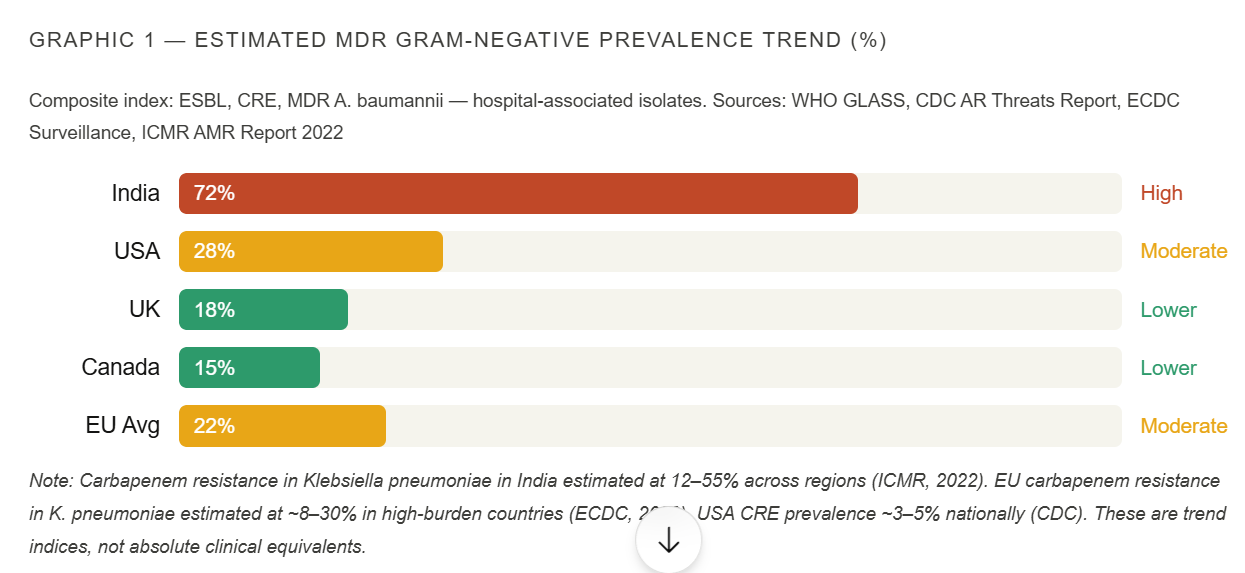
AMR is a global crisis — no country is exempt. But the distribution of multidrug-resistant (MDR) pathogens is not uniform. South Asia, including India, bears a disproportionate burden of gram-negative MDR organisms, particularly carbapenem-resistant Enterobacteriaceae (CRE), extended-spectrum beta-lactamase (ESBL)-producing organisms, and MDR Acinetobacter baumannii.
The following comparison is grounded in surveillance data from WHO, CDC, ECDC, and ICMR. These figures represent estimated community and healthcare-associated AMR prevalence trends rather than single-point clinical trial values — methodology and surveillance intensity differ significantly across countries.
The Perception Challenge: NDM and the Global Narrative
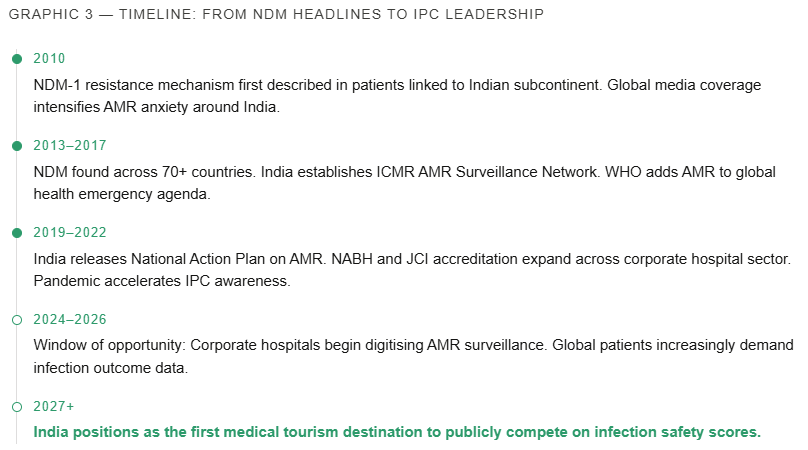
No discussion of AMR and India can avoid the New Delhi Metallo-beta-lactamase (NDM-1) story. When this resistance gene was first described in 2010 in patients linked to the Indian subcontinent, the clinical and media response was immediate — and the reputational damage to India’s healthcare sector was significant and lasting.
It is scientifically important to be precise here. NDM-1 is a globally disseminated resistance mechanism. It is now detected in patients across Europe, North America, Africa, and Southeast Asia — many with no prior connection to the subcontinent. The gene is carried on mobile genetic elements (plasmids) that spread horizontally across bacterial species. It is a global problem that carries a geographical name.
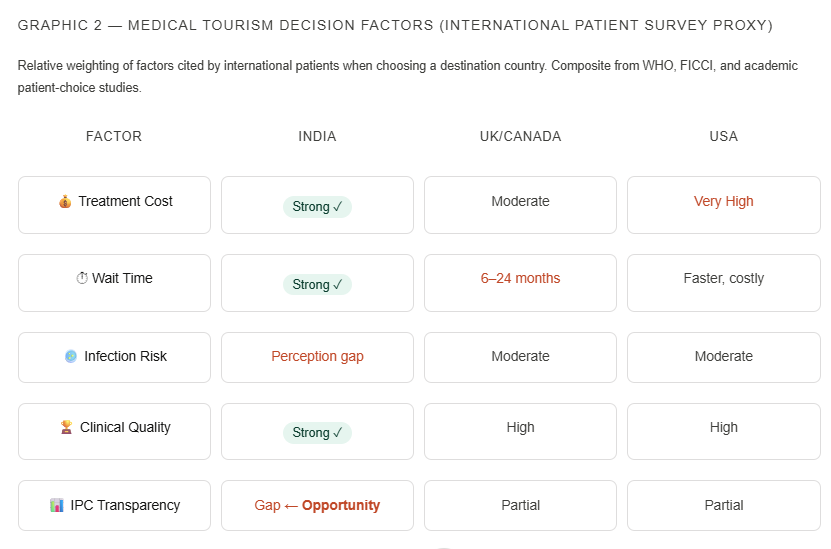
But perception shapes reality in medical tourism. Academic studies and patient surveys consistently show that infection risk — especially AMR — is among the top three concerns for patients considering medical travel to South Asia. Fear of acquiring a resistant infection during hospitalization acts as a silent veto: patients who would otherwise choose India for orthopaedics, cardiac surgery, or oncology quietly redirect to Thailand, Turkey, or Malaysia instead.
India’s Competitive Strengths Are Formidable — One Pillar Is Missing
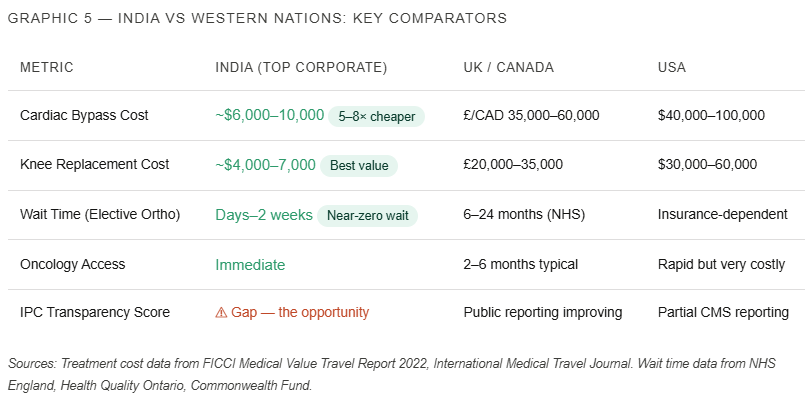
Let us be direct about what India’s top-tier corporate hospitals already offer. The clinical talent is genuinely world-class: Indian-trained cardiac surgeons, oncologists, transplant teams, and orthopaedic specialists operate at skill levels that match any major Western centre. The English-speaking healthcare ecosystem, streamlined administrative pathways, and the ability to schedule complex procedures within days — not months — create an offer that is objectively superior to many high-income country alternatives.
India already wins decisively on affordability, speed, and clinical capability. The missing pillar — the one that could unlock the next tier of international patient inflow — is internationally trusted infection safety.
The Strategic Thesis: IPC Excellence as a Medical Tourism Brand
The hospitals that will win the next phase of global medical tourism are those that treat Infection Prevention & Control (IPC) not as a regulatory compliance function, but as a strategic brand asset and revenue multiplier.
The mechanism is straightforward. An international patient researching cardiac surgery abroad today has access to a growing volume of online information, patient forums, and clinical outcome databases. When they search for infection safety data about Indian hospitals, they find almost nothing publicly available — not because outcomes are necessarily poor, but because the data is not published. This absence of evidence is interpreted, rationally, as evidence of absence of quality.
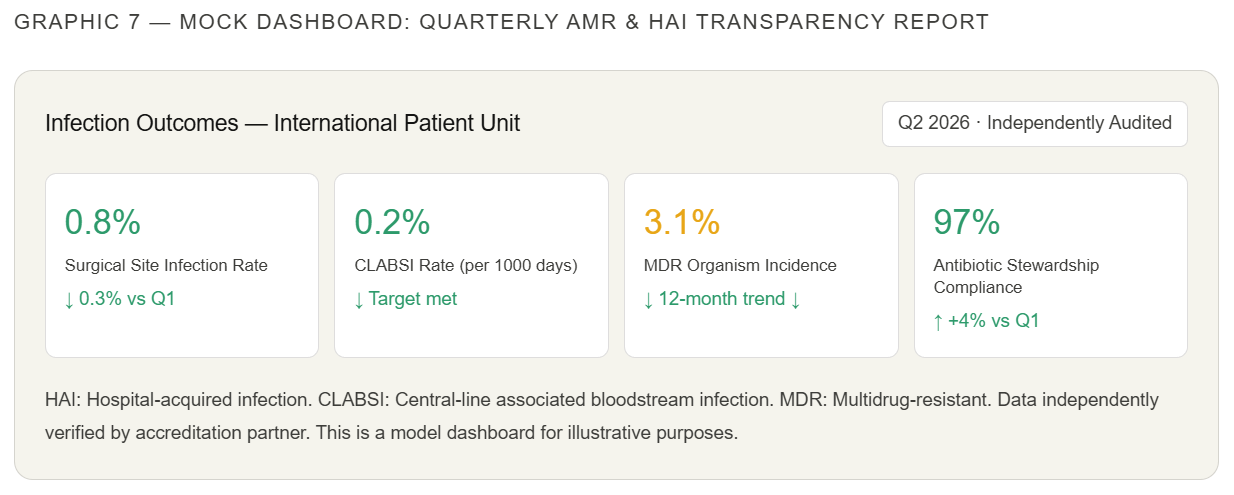
The solution is transparent, independently audited AMR surveillance reporting. Here is what that looks like in practice:
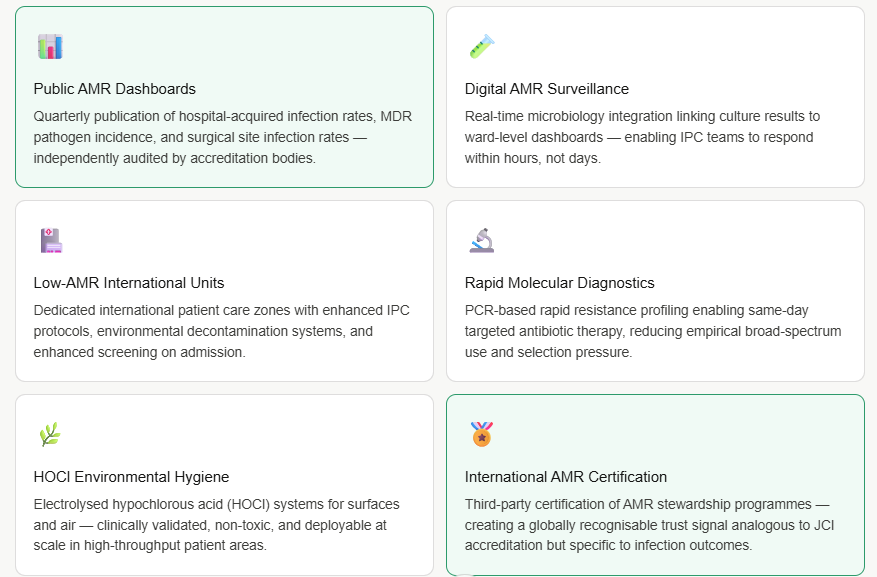
Publicly reporting lower AMR rates must be independently audited and evidence-based. The credibility of this entire strategy rests on the integrity of the data. Self-reported, unverified infection statistics will not be trusted by international refer
India’s Strategic Vision: Compete on Safety, Not Just Price
The strategic vision is this: India becomes the first major medical tourism destination in the world to openly, publicly compete on infection safety outcomes. Not to claim perfection — no system anywhere achieves that — but to demonstrate measurable, consistent, improving infection control performance with the kind of transparency that international patients, insurance partnerships, and referring physicians can evaluate.
The infrastructure elements of this vision are achievable within a 3–5 year horizon for India’s leading corporate hospital groups:
First, AI-enabled infection surveillance systems that integrate microbiology, pharmacy, and ward data — identifying resistant organism clusters in real time and triggering IPC protocols before outbreaks develop. Second, smart architectural isolation: purpose-designed international patient facilities, ideally adjacent to major airport hubs in Delhi, Mumbai, Hyderabad, Bengaluru, and Chennai, incorporating UV-C automated room disinfection, positive/negative pressure zone switching, and HOCl-based continuous surface and air decontamination. Third, a government-supported “Safe Care India” initiative — akin to a public quality mark — that certifies hospitals meeting defined IPC and AMR stewardship benchmarks, promoting them as verified safe destinations for international patients. This initiative would be supervised by a joint ICMR-NABH-Ministry of Tourism body and open to independent international audit.

A Call to Leaders: IPC Is Economic Strategy
To corporate hospital CEOs, hospital chains, healthcare investors, NABH and JCI accreditation leaders, infection control committees, and policymakers — the message is this: IPC and AMR transparency are not compliance burdens. They are national healthcare infrastructure, reputation capital, and economic strategy simultaneously.
Every percentage point reduction in hospital-acquired MDR infection rates is a clinical outcome, a patient safety achievement, a financial improvement (resistant infections extend length of stay by an average of 6–21 additional days), and a marketing asset — if you measure it, audit it, and publish it.
The international patient who chooses India over Thailand or Turkey because they have seen your infection outcome data — independently verified, consistently improving — is a patient who will return, who will refer family and colleagues, and whose choice generates not just revenue but national healthcare reputation.
The window to lead this transformation is open now. The hospitals that move first will not just benefit commercially. They will have earned the right to say: we changed how the world sees Indian healthcare.
Key Citations
Murray CJ et al. (2022) Global burden of bacterial antimicrobial resistance. The Lancet. |
ICMR AMR Surveillance Network Annual Report 2022. |
WHO Global Antimicrobial Resistance and Use Surveillance System (GLASS) Report 2022. |
CDC Antibiotic Resistance Threats in the United States, 2019. |
ECDC Antimicrobial Resistance in the EU/EEA (EARS-Net), 2022. |
FICCI Healthcare: Medical Value Travel Report 2022. |
Commonwealth Fund International Health Policy Survey. |
NHS England Referral to Treatment Statistics.
Note: All comparative AMR prevalence data should be interpreted in the context of differing surveillance systems, reporting intensity, and clinical settings across countries. Figures cited represent trend indices from peer-reviewed and institutional surveillance sources, not direct clinical equivalents.
Leave a Reply