
Disinfectant-Tolerant Bacteria: A Contamination Threat in Hospital Environments and Onsite HOCl Generation as an Effective Control Strategy
The Rising Threat: Disinfectant-Tolerant Bacteria
Several bacterial species are developing resistance to common disinfectants — adding a dangerous new layer to an already complex antimicrobial resistance landscape. The mechanisms mirror antibiotic resistance: selective pressures drive vertical and horizontal gene transfer via mobile genetic elements, passing resistance from a dwindling population of tolerant bacteria to previously susceptible strains.
Two disinfectant classes are of particular concern: • Quaternary Ammonium Compounds (QACs) — including benzalkonium chloride, the most widely used hospital surface disinfectant globally. qac genes, especially qacEΔ1, confer resistance via efflux pump upregulation, reducing intracellular disinfectant concentration below lethal thresholds. • Biguanides — including chlorhexidine, the cornerstone antiseptic for skin preparation, patient bathing, and hand hygiene in virtually every hospital worldwide.
What is Happening Inside Hospitals? New 2026 Evidence
New research from Northwestern University (2026) has brought the scale of this problem into sharp focus. Chlorhexidine — in clinical use for over 70 years — is now at the centre of a contamination control crisis that extends well beyond the skin surface where it is applied.
Residues Linger, Tolerance Builds In laboratory experiments simulating hospital cleaning, chlorhexidine was applied to common hospital surface materials: plastic, metal, and laminate. Even after treatment with chlorhexidine-free disinfectants, residues persisted beyond 24 hours at concentrations of ≥18.75 μg/mL — too low to kill, but sufficient to exert selective pressure. Under these sub-lethal conditions, bacteria survived, adapted, and developed tolerance.
Organisms demonstrating resistance included:
- Pseudomonas aeruginosa — opportunistic pathogen, high risk in ICU settings
- Stenotrophomonas maltophilia — intrinsically resistant to many antibiotics
- Elizabethkingia miricola — an emerging pathogen from an entirely different phylum Minimum inhibitory concentrations reached up to 512 μg/mL. The primary resistance mechanism identified: qacEΔ1-carrying, plasmid-borne multidrug-resistant cassettes — confirming that mobile genetic resistance elements link disinfectant and antibiotic resistance.
“For immunocompromised patients and critically ill ICU populations, disinfectant resistance is not an abstract microbiology concern — it is a direct, life-threatening patient safety risk.”
Quaternary Ammonium Compounds (QAC): A Parallel Resistance Crisis
Benzalkonium chloride — the archetypal QAC disinfectant — is used on virtually every hospital surface. It acts by disrupting bacterial cell membranes through electrostatic interaction. However, bacteria have evolved a well-documented counter-response.
The qac gene family (qacA, qacB, qacC, qacEΔ1) encodes membrane-associated efflux pumps that actively expel the quaternary ammonium compound before it reaches effective intracellular concentrations. These genes are predominantly plasmid-borne, enabling rapid horizontal transfer.
Of particular concern: cross-resistance. Bacteria harbouring qac-mediated efflux systems also display reduced susceptibility to structurally dissimilar antibiotics — including ciprofloxacin, trimethoprim, and chloramphenicol. The routine use of QAC disinfectants may thus be inadvertently selecting for multidrug antibiotic resistance in the hospital environment.
The overuse and misuse of single-mechanism disinfectants — both QACs and chlorhexidine — is the primary driver behind the emergence of disinfectant resistance. The solution must address the mechanism of failure, not just the symptom
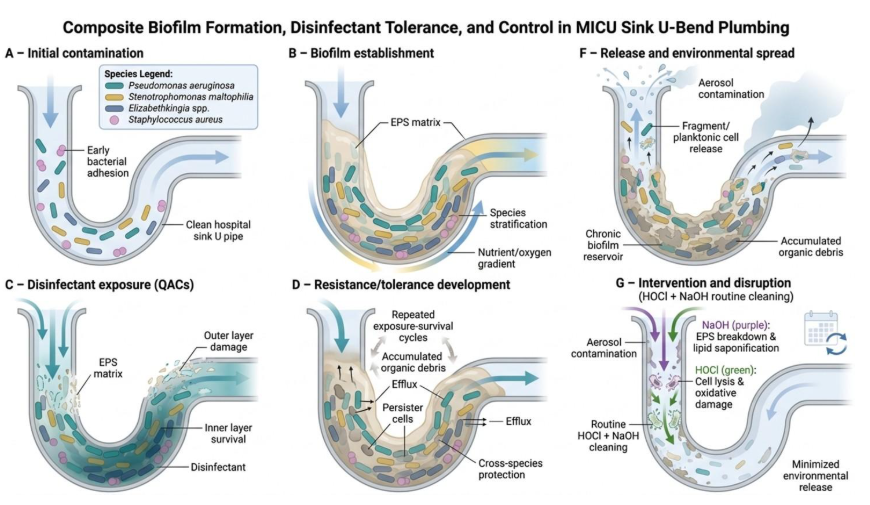
Sink Drains: The Biggest Hotspot
From 200 MICU samples — collected from bed rails, keyboards, door sills, light switches, and sink drains — researchers isolated over 1,400 bacteria. Critically, 36% exhibited some level of chlorhexidine tolerance.
Sink drains stood out as the highest-concentration reservoir. The P-trap — the U-shaped pipe beneath the sink that retains a small volume of water — creates an ideal environment for antimicrobial-resistant biofilm formation. Each time water flows, aerosols are generated, carrying resistant organisms into the room environment.
Tolerant bacteria were recovered even from the tops of door frames, confirming airborne transmission as a genuine and underappreciated route of exposure.
“The clinical implication is stark: standard surface decontamination does not neutralise the drain reservoir. Airborne pathways must now be incorporated into hospital contamination control risk assessments”.
The Solution: Onsite HOCl Generation
Why HOCl Is Resistance-Proof
Hypochlorous acid (HOCl), generated onsite through electrochemical activation of salt water, addresses this problem at its fundamental root — because resistance to HOCl is, in practical terms, impossible.
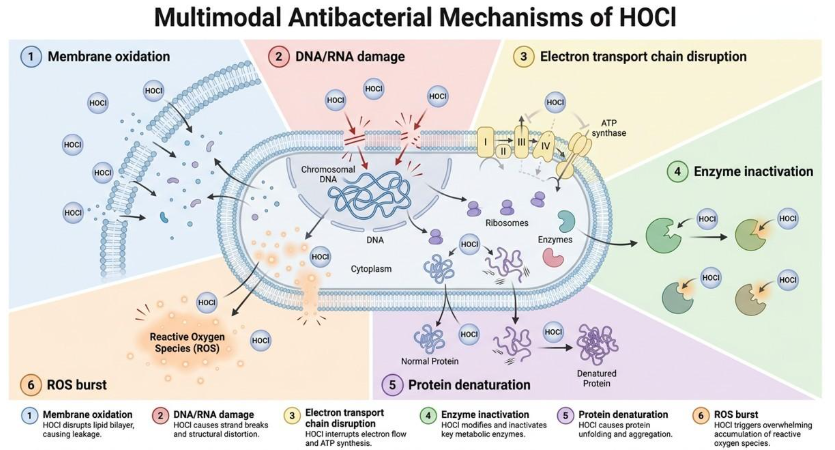
Unlike chlorhexidine or benzalkonium chloride, which act via a single primary mechanism, HOCl attacks bacteria through simultaneous, multiple mechanisms:
- Oxidative destruction of cell membranes — direct structural breach
- Irreversible enzyme inactivation — metabolic collapse
- DNA and RNA disruption — No gene transfer dead or alive
- Protein denaturation — structural and functional proteins destroyed
- Disruption of electron transport chains — energy production eliminated • Overwhelming reactive oxygen species (ROS) burst — systemic oxidative stress
No bacterium can simultaneously develop resistance to all these mechanisms. There is no single gene transfer event, no plasmid, no efflux pump that can neutralise a simultaneous multi-front oxidative assault. This is why HOCl has been deployed by the human immune system — produced by neutrophils — for millions of years, and no pathogen has ever evolved durable resistance to it.
No qac genes. No MIC creep. No tolerance build-up from residue accumulation. HOCl leaves no sub-lethal residue — it degrades to harmless saline — eliminating the selection pressure that creates tolerance in the first place.
The NaOH Byproduct: Solving the P-Trap Problem
Onsite HOCl generation via electrolysis of sodium chloride solution produces sodium hydroxide (NaOH) as an unavoidable co-product. Rather than treating this as waste, the NaOH stream can be directly deployed into sink drains and P-traps — where this study identified the highest concentration of resistant organisms.
NaOH is precisely suited to this application:
- Dissolves biofilm matrices within drain pipework at their organic matrix level
- Saponifies grease and organic matter that sustains resistant organisms
- Maintains continuous drain hygiene between deep-cleaning cycles
- Significantly reduces the bacterial load available for aerosol generation at each use.
This transforms a chemistry by-product into a targeted drain decontamination tool — addressing the single largest reservoir identified in the Northwestern MICU study, without any additional chemical procurement or logistics.
Broader Implications for Infection Control Strategy
The findings from the Northwestern study, combined with the growing literature on QAC and chlorhexidine resistance, deliver a clear message for infection control professionals:
- Disinfectant rotation programmes must now account for residue persistence, not just surface kill rates at point of application
- Environmental monitoring must include sink drains as high-priority sampling sites, with routine biofilm surveillance
- Airflow pathways must be incorporated into contamination control risk assessments — airborne transmission of resistant organisms from drains is documented
- Single-mechanism disinfectants create evolutionary selection pressure — multi-mechanism alternatives must be prioritised
- Onsite HOCl generation represents an infrastructure-level decision with both clinical and pharmacoeconomic advantages: no supply chain, no residue, no resistance
Conclusion
Disinfectant resistance — driven by QAC-associated qac genes and chlorhexidine tolerance mechanisms — is no longer a theoretical concern. It is present, measurable, and spreading through hospital environments via both contact and airborne routes. The P-trap drain is the primary reservoir; sub-lethal residue exposure is the primary driver.
Onsite HOCl generation offers a scientifically sound, operationally practical response: a resistance-proof disinfectant with simultaneous multi-mechanism bactericidal action, and a co-produced alkaline byproduct that directly addresses the drain reservoir. It is not a niche technology — it is the next logical step in hospital contamination control infrastructure.
Key References
- Shen J, et al. Hospital Environments Harbor Chlorhexidine-Tolerant Bacteria. Environmental Science & Technology, 2026. DOI: 10.1021/acs.est.5c18587
- Vijayakumar R & Sandle T. Biocide reduced susceptibility due to plasmid-borne antiseptic-resistant genes. J Applied Microbiology, 2019; 126(4): 1011-1022.
- Partridge SR, et al. Mobile Genetic Elements Associated with Antimicrobial Resistance. Clin Microbiol Rev, 2018. DOI: 10.1128/cmr.00088-17
- Lipworth S, et al. The plasmidome associated with Gram-negative bloodstream infections. Nat Commun, 2024; 15: 1612.
- McCarlie S, Boucher C, Bragg R. Molecular basis of bacterial disinfectant resistance. Drug Resistance Updates, 2020; 48. DOI: 10.1016/j.drup.2019.100672
- Cole K & Talmadge JE. Mitigation of microbial contamination from wastewater and aerosolization by sink design. J Hosp Infect, 2019; 103(2): 193-199.
Leave a Reply